The Machine in Kisumu: How a Sickle-Cell Treatment Routine Abroad Finally Reached Kenya's Warriors
For Kenyans living with sickle cell — and the diaspora families who quietly fund their care from abroad — a public hospital's first apheresis machine narrows a gap that has lasted generations.
In a treatment room at the Jaramogi Oginga Odinga Teaching and Referral Hospital in Kisumu, Mitchelle Omullo lay beside a softly humming machine and watched her own blood travel out of her arm, through a tangle of clear tubing, and back again. She had spent most of her life bracing for the next crisis — the deep bone pain, the exhaustion, the fear that arrived with every fever. After surviving two mild strokes, she had begun to believe her body was simply running out of room. This was something different. This was a machine doing, in a few hours, what years of pills and prayer had not managed: giving her a reason to expect more good days than bad ones.
Omullo, diagnosed with sickle cell disease at the age of three, became the first patient to undergo an automated red blood cell exchange at a Kenyan public hospital. The procedure was delivered at JOOTRH in collaboration with Nairobi West Hospital, and for the community of Kenyans who call themselves "warriors," it carried a weight far beyond one woman's recovery. For decades, this was the treatment they read about happening somewhere else — in London wards, in American clinics, in the hospitals where their relatives abroad were quietly cared for.
What the machine actually does
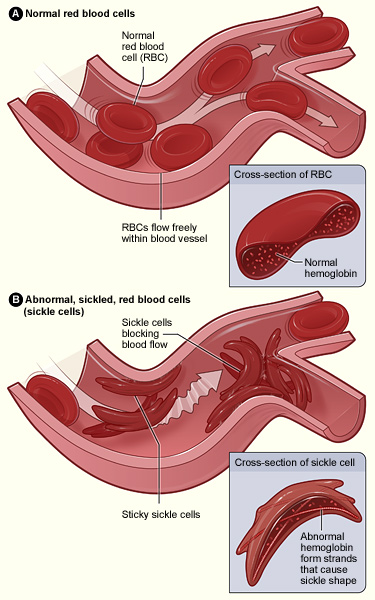
Automated red blood cell exchange, or RBCx, is a form of apheresis. A patient is connected to a machine that draws out their blood, separates the defective, crescent-shaped red cells that define sickle cell disease, and returns the healthy components — plasma and platelets — along with donor blood. The goal, as clinical haematologist Dr Boniface Kairu describes it, is to bring the proportion of sickled blood in circulation down from nearly 100 per cent to somewhere around 25 to 30 per cent.
That single shift can change the arithmetic of the disease. When healthy blood is allowed to flow freely, the catastrophic complications — strokes, chronic leg ulcers, the acute chest crises that fill emergency wards — become far less likely. Dr Kairu says he has watched ulcers heal and hospital admissions fall sharply among patients who receive the procedure regularly, with measurable gains in their quality of life.
The benefit, however, is not permanent. Transfused blood has a working life of roughly three months, after which the exchange must be repeated to hold the line. RBCx is also not a starting point. Most patients, Dr Kairu notes, can be managed for years on simpler, cheaper interventions — hydroxyurea, folic acid and penicillin — and earlier diagnosis means many more Kenyans now live with the condition into adulthood. The machine is for the severe cases, the warriors whose crises come too often and cut too deep.
A gap the diaspora has always known
Sickle cell disease is not a distant or exotic illness for the Kenyan diaspora. It is, in many ways, the condition that travels with them. The World Health Organization estimates that 7.74 million people were living with the disease globally in 2021, and that some 515,000 babies were born with it that year — close to 80 per cent of them in sub-Saharan Africa. The genetic trait that causes it followed the African diaspora across oceans and centuries, which is why sickle cell remains one of the most common inherited blood disorders among Black communities in the United States, the United Kingdom and beyond.
What differed, until now, was access. In the hospitals of Houston, Atlanta, London and Birmingham, automated exchange has long been routine — a standard tool for managing severe disease and preventing strokes, available on demand. Kenyan families with relatives abroad knew this. They heard about the procedure in phone calls and WhatsApp groups, watched a cousin in Maryland or an aunt in Manchester receive care that simply did not exist back home, where treatment too often meant managing pain rather than preventing it. The arrival of RBCx in a public hospital in Kisumu does not erase that gap, but it begins, for the first time, to close it on Kenyan soil.
The money question — and where remittances come in
The harder truth sits in the economics. Selina Olwanda, chief executive of the Children Sickle Cell Foundation, welcomes the new technology but is blunt about the obstacle that outlasts any single machine: cost and access. A treatment that must be repeated every three months is, for many families, an expense without end. Even with the cushion of universal health coverage, she says, the repeat nature of the procedure makes it overwhelming for households already stretched by years of medical bills.
This is precisely the seam where the diaspora's role becomes visible. Kenya's first national remittances survey, released this month, found that families abroad sent home some Ksh931.8 billion over a single year, with the United States accounting for the largest share at 43.5 per cent. Crucially, medical expenses were among the biggest uses of that money, at close to a quarter of all remittance spending. For a sickle cell family, the difference between a child who receives a quarterly exchange and one who does not may come down to whether a parent or sibling overseas can keep covering the cost. The machine in Kisumu and the money wired from a hospital cafeteria in New Jersey are, increasingly, part of the same care plan.
Access, geography and what comes next
Kenya carries a heavy burden. The Ministry of Health estimates that roughly 14,000 children are born with sickle cell disease in the country each year, and that about 18 per cent of the population carries the trait, with the highest concentrations in the Nyanza, Western and Coastal regions. In the Lake Region alone, around 4,000 babies are born with the condition annually — which makes the choice of Kisumu, in the heart of that burden, more than symbolic.
Yet Olwanda warns that a single advanced machine cannot substitute for a working system beneath it. Where a patient lives still largely determines the care they receive; those in cities fare better than those in rural areas. Real progress, she argues, depends on strengthening the primary health facilities that catch the disease early, monitor it closely and prevent the crises that send people toward specialised treatment in the first place. If those frontline clinics were properly equipped, fewer patients would ever need the apheresis room.
For now, the warriors are choosing hope carefully. Omullo, who founded the West Kenya Sickle Cell Organisation and produced a documentary on the disease titled Ray of Hope, says the procedure changed her life and is urging others with severe crises to consider it. Her case is one patient, one machine, one hospital. But for a diaspora that has spent years watching this treatment happen everywhere except home, it is the first sign that the distance is finally beginning to shrink.



