The Doctor Who Carried It Across Borders: How Congo's Ebola Outbreak Reached Kinshasa, Uganda, and a Watching Diaspora
A virus with no vaccine has killed hundreds in eastern Congo, slipped into Uganda, and forced a capital of 18 million to ban crowds. East Africa's diaspora is watching the map.
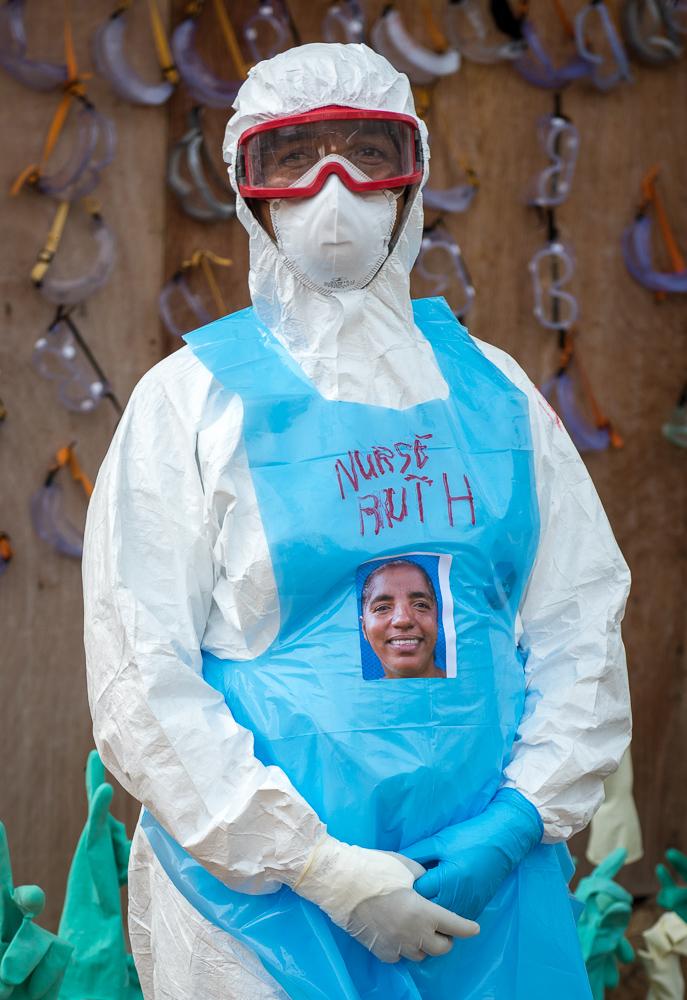
He had spent his days in one of the towns at the centre of an epidemic, working inside an Ebola treatment centre where the virus is closest and the protective suits never come off for long. Then he travelled home. His route took him through Kinshasa, the Democratic Republic of Congo's vast capital, before he continued on to France, where a test came back positive.
That single journey — from an eastern treatment ward, through a city of eighteen million people, and on to another continent — is the reason a public-health emergency that had been confined to remote provinces suddenly felt, this week, as though it could be anywhere. The day after the doctor's case became public, the Congolese government ordered a 21-day quarantine for anyone travelling from Ebola-affected areas to other parts of the country. For families across East Africa and for the diaspora that watches home from a distance, the message was unmistakable: a virus moves the way people move.
A Ban That Reached the Capital
On Saturday, Interior Minister Jacquemain Shabani banned mass gatherings in Kinshasa and in three other provinces — Tshopo, Haut-Uele and Bas-Uele — all of which border the regions where Ebola has been confirmed. No cases have yet been recorded in the capital itself. But authorities, mindful of how quickly the disease can travel and how dense the city is, chose to act before rather than after.
The decision landed in the middle of a political season. Prominent opposition figures accused the government of using public health as cover to smother dissent, pointing to a protest march scheduled for 8 July. Prince Epenge, a spokesperson for the Lamuka coalition, told the BBC the order was "not legitimate." Rodrigue Ramazani of the Envol party urged supporters to ignore it, calling the directive a "political manoeuvre rather than a public health measure." The march had been organised against a proposed law that critics say could allow President Felix Tshisekedi to remain in power beyond his two-term limit. The government did not respond to the criticism.
For ordinary Kinshasa residents, the dispute is more than abstract. A gathering ban touches funerals, markets, churches and weddings — the texture of daily life — and it does so in a country where trust between citizens and the state is already thin. That tension, between the genuine need to slow a deadly virus and the suspicion that emergency powers can be bent to other ends, is one the region has lived through before.
The Numbers Climbing in the East
The outbreak itself remains roughly 1,800 kilometres from the capital, concentrated in three eastern provinces: Ituri, North Kivu and South Kivu. Ituri is by far the worst hit, accounting for more than nine in ten infections. Mass gatherings there have been banned for weeks.
When the interior minister issued his order, confirmed cases across the affected provinces had jumped by 47 in a single update, bringing the total to 1,274, with 360 known deaths. By the following day, other international outlets were reporting still higher figures — more than 1,300 cases and over 370 deaths — a reminder that the count is a moving target rather than a settled tally.
What makes this outbreak particularly worrying to epidemiologists is its cause. It is driven by the Bundibugyo species of the virus, for which there is currently no approved vaccine. Both the Africa Centres for Disease Control and Prevention and United States public-health authorities have warned that the outbreak has the potential to become one of the largest ever recorded, in large part because the virus was circulating undetected for weeks before it was confirmed to be Ebola. A pathogen that spreads quietly is one that has a head start.
Across the Border, Into Uganda
The number that should focus East African minds is a smaller one. Across the border in Uganda, the World Health Organization says twenty people are known to have been infected, and two deaths have been confirmed.
Uganda is not a distant abstraction. It is a member of the East African Community, Kenya's western neighbour, and a country bound to its surroundings by roads, trade, family ties and the constant movement of people. An outbreak that crosses from Congo into Uganda is no longer somebody else's problem on the far side of a rainforest; it is a regional one, edging closer to Nairobi, Kampala and the border towns that stitch the region together. The same porousness that makes East Africa a single economic space also makes it a single epidemiological one.
It is why the Congolese quarantine order, and the story of the doctor who passed through Kinshasa before testing positive abroad, resonate well beyond Central Africa. Health security here is not contained by national lines on a map.
What the Diaspora Sees From Afar
For East Africans living in London, Toronto, Doha or Atlanta, an outbreak at home is followed with a particular kind of attention — the worry of distance, sharpened by the knowledge that one cannot simply get on a plane and check. Parents and siblings remain in the affected region or in neighbouring countries. Quarantine rules and travel advisories complicate the routine trips home that anchor diaspora life. And every headline raises the quiet calculation of when, and whether, it is safe to visit.
The diaspora also has a professional stake. East African nurses, doctors and lab scientists are woven into the health systems of the Gulf, Britain and North America; many trained in the same regional institutions now mobilising against the virus. They read these bulletins not only as worried relatives but as practitioners who understand exactly what a Bundibugyo outbreak with no vaccine demands of the colleagues they left behind. When the diaspora sends money home during a health crisis, it is often this knowledge — of what a treatment centre actually needs — that guides where the help goes.
The Race for a Treatment, Amid a War
There is a thread of hope. The head of the Africa CDC told the BBC that trials for new antiviral drugs could begin as soon as this week, a faster timeline than past outbreaks allowed. Science, for once, may move at something closer to the speed of the virus.
But the response is unfolding in one of the hardest places on earth to mount one. The WHO has warned that conflict in eastern Congo is making the outbreak far more difficult to contain. The M23 rebel group controls large parts of both North and South Kivu — precisely the provinces where the disease is spreading — leaving health workers to trace contacts and isolate the sick across front lines and in communities exhausted by years of violence.
That is the uncomfortable truth beneath the case counts. Ebola is a medical emergency, but stopping it is a political and logistical one, dependent on trust, access and stability that are all in short supply. For now, the capital has closed its crowds, the borders are watching their travellers, and a diaspora scattered across the world is watching the map — hoping the next number it reads is one that has finally stopped climbing.



